Decompensated liver disease
This is an online E logbook to discuss our patients' de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from the available global online community of experts intending to solve those patients clinical problems with the collective current best evidence-based inputs. This e-log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box are welcome.
A 27yr old male patient resident of Nalgonda came with
CHIEF COMPLAINTS-
C/o loss of appetite since 20 days
C/o blood in urine since 10 days and
C/o pedal edema since 10 days
HISTORY OF PRESENT ILLNESS-
Patient was apparently asymptomatic 20 days back then he had loss of appetite for which he went to the hospital and was diagnosed as CLD spleenomegaly and portal hypertension for which he took medication after which he developed haematuria since 10 days and pedal oedema which is of pitting type. grade 1
Pedal edema is relieved by taking rest and increases on walking. Malena 20days ago for 10 days.
He complained of decreased sleep since 1 month.
No c/o abdominal pain, vomiting, loose stools,burning micturition.
HISTORY OF PAST ILLNESS-
He had similar complaints in the past (1 yr ago)
Not a known case of DM, HTN, Epilepsy, TB, CVA, CAD.
SURGICAL HISTORY-
H/o appendectomy 4 yrs back.
PERSONAL HISTORY-
Appetite- lost since 20 days
Non-vegetarian
Bowels- regular
Micturition- haematuria since 10 days
Addictions-
Alcohol- regularly since the past 6 yrs. increased intake since last 2yrs. 1/2 bottle per day twice daily
FAMILY HISTORY-
Father is a chronic alcoholic.
PHYSICAL EXAMINATION-
GENERAL EXAMINATION-
Pallor- No
Icterus- yes
Cyanosis-No
Clubbing- yes
Lymphadenopathy- No
Odema of feet- yes (grade 1)
Temperature-afebrile on touch
Pulse rate- 90/ min
Respiration rate-20/min
Blood pressure-100/60 mm hg
SYSTEMIC EXAMINATION-
CVS-
Thrills- No
Cardiac sounds- s1s2 heard
Cardiac murmurs- No
RESPIRATORY SYSTEM-
Dyspnoea- No
Wheeze- No
Breath sounds -vesicular
ABDOMEN-
Inspection:
Shape of abdomen- scaphoid
skin- no scars, striae
Flanks – free
umbilicus-central inverted
no dilated veins
movements of abdominal wall-normal
hernial orifices with cough impulse- normal
Palpation:
local rise in temperature -absent
Tenderness- not present
Palpable mass- not present
Free fluid- not present
Liver and spleen not palpable
Percussion
fluid thrill absent
liver span-17cm
spleen -normal
Auscultation:
bowel sounds- 14/min
bruits- normal
CNS-
Level of consciousness- consciousness
Speech- normal



INVESTIGATIONS-
HEMOGRAM
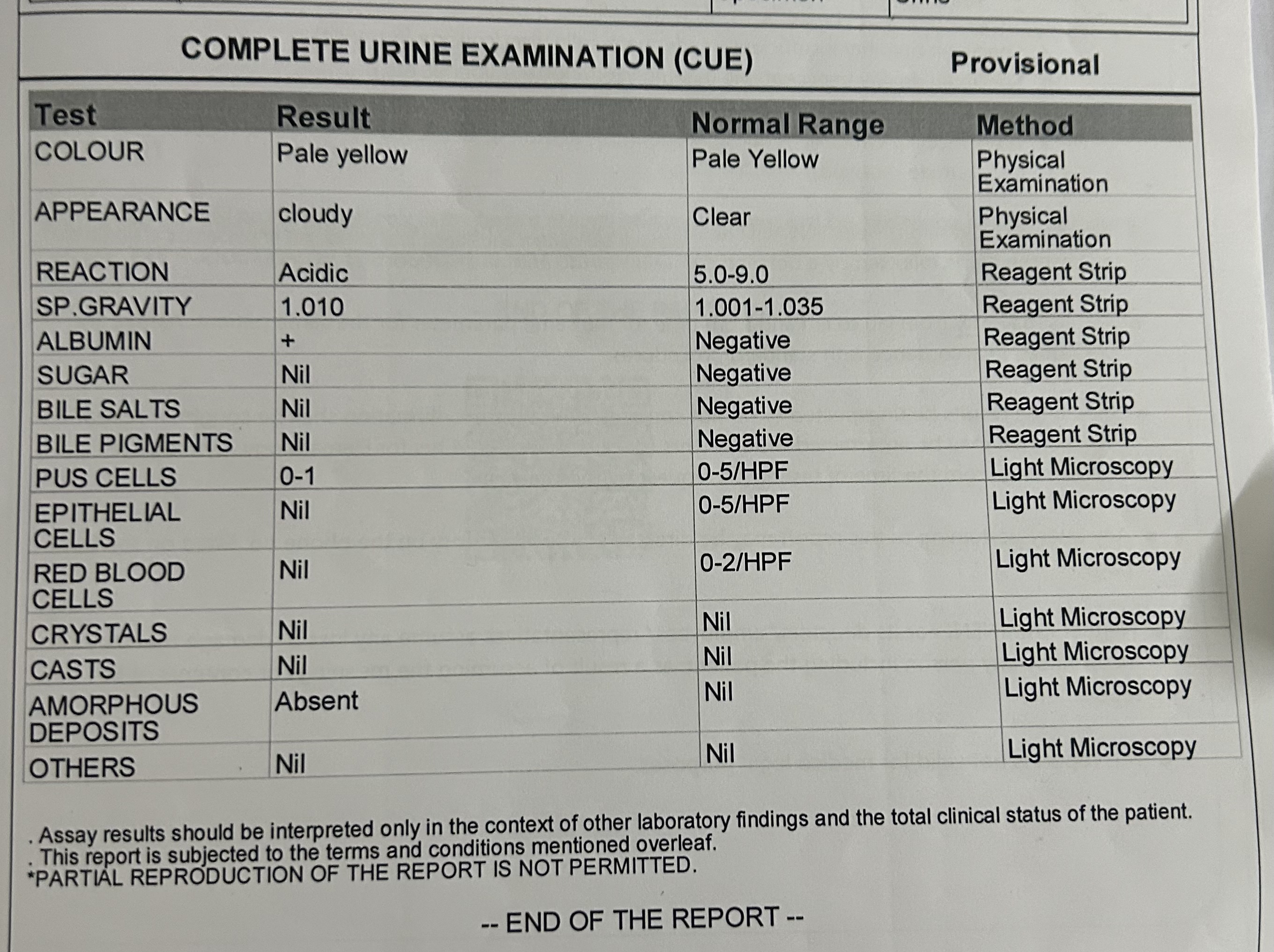
CUE
APTT
PROTHROMBIN TIME
BLOOD SUGAR- RANDOM
BLOOD UREA
SERUM CREATININE
SERUM ELECTROLYTES AND SERUM CALCIUM
LIVER FUNCTION TESTS
ULTRASOUND









PROVISIONAL DIAGNOSIS-DECOMPENSATED LIVER DISEASE - grade 1 ( hepatic encephalopathy)
HYPOTONIC HYPONATREMIA - diuretic induced.
TREATMENT-
Rx
IV fluids NS 75ml/hr
Inj vitamin K 10 mg IV/OD
Inj Thiamine 200 mg IV/BD in 100 ml NS
T Doxy 100 mg PO/BD
T Udiliv 300 mg PO/ BD
T Viboliv 500 my PO/BD
Syp. Hepamerz PO/T/ID


Comments
Post a Comment